Post Traumatic Stress Disorder Research
Urine Testing
Reveals low levels of cortisol which "suggests a physiological adaptation of the hypothalamic-pituitary-adrenal axis to chronic stress."
J Nerv Ment Dis 1990 Jun;178(6):366-
Low urinary cortisol excretion in Holocaust survivors with posttraumatic stress disorder compared to Holocaust survivors without ptsd. Personally I had a difficult time imagining a survivor of the Holocaust without PTSD.
"...low cortisol levels may persist for decades following exposure to trauma among individuals with chronic PTSD."
Am J Psychiatry. 1996 Jun;153(6):846.
"Increased 24-hour urinary cortisol excretion in patients with post-traumatic stress disorder and patients with major depression, but not in patients with fibromyalgia."
Acta Psychiatr Scand 1998 Oct;98(4):328-35
The results of our study suggest that initial cortisol levels in the immediate aftermath of a traumatic event contribute, in part, to subsequent symptoms of posttraumatic stress disorder.
Biol Psychiatry 2000 Nov 1;48(9):940-7
Behavioral Therapy
CBT: Cognitive Behavior Therapy
Open-label trial of cognitive behavior therapy for insomnia and disturbing dreams in crime victims with PTSD. There was significantly greater improvement.
Am J Psychiatry 2001 Dec;158(12):2043-7
Cognitive-behavior therapy vs exposure therapy in the treatment of PTSD in refugees. Both forms of therapy were provided and they were equally very helpful in reducing anxiety and depression in the PTSD refugees.
Behav Res Ther 2001 Oct;39(10):1183-97
Virtual Reality Exposure Therapy for Vietnam Vets
Virtual reality exposure therapy for Vietnam veterans with posttraumatic stress disorder. Study revealed this form of therapy is very successful in treating Vietnam veterans.
J Clin Psychiatry 2001 Aug;62(8):617-22
Imagery Rehearsal Therapy
"Imagery rehearsal therapy for chronic nightmares in sexual assault survivors with posttraumatic stress disorder: a randomized controlled trial... Imagery rehearsal therapy is a brief, well-tolerated treatment that appears to decrease chronic nightmares, improve sleep quality, and decrease PTSD symptom severity."
JAMA. 2001 Aug 1;286(5):584-8.
EMDR
Eye movement desensitization and reprocessing (EMDR): a meta-analysis.
This article reveals that EMDR was evaluated in 34 studies and it was found to be an effective treatment for non-combat PTSD but it no more effective than other exposure techniques "and evidence suggests that the eye movements integral to the treatment, and to its name, are unnecessary."
J Consult Clin Psychol 2001 Apr;69(2):305-16
Drug Therapy
Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study.
"Doses of 20 and 40 mg/day of paroxetine are effective and well tolerated in the treatment of adults with chronic PTSD."
Am J Psychiatry 2001 Dec;158(12):1982-8
Efficacy of sertraline in preventing relapse of posttraumatic stress disorder: results of a 28-week double-blind, placebo-controlled study.
The study showed that sertraline did provide protection against relapse and provided evidence of improvement in PTSD symptoms.
Am J Psychiatry. 2001 Dec;158(12):1974-81.
Topiramate in posttraumatic stress disorder: preliminary clinical observations.
Topiramate was tested on 3 PTSD patients and it reduced and even eliminated "trauma-related intrusive memories and nightmares and normalizing depressed mood" in these patients. The study says that further study of this anti-epileptic medication for PTSD is warrented.
J Clin Psychiatry 2001;62 Suppl 17:60-3
Chemical Dependency
"An estimated 30% to 50% of cocaine-dependent individuals meet criteria for lifetime PTSD."
J Subst Abuse Treat 2001 Jul;21(1):35-45
More to Come!
http://www.mhsanctuary.com/ptsd/research.htm
Monday, August 27, 2007
Pace: Psychological Wounds Need Same Attention As Physical Wounds
A Soldier's Mind
“The program has done a lot for me and my family,” said a Marine veteran of the second battle for Fallujah. “I didn’t believe there was anything wrong with me when I came back to Kaneohe Baby. By the time I did, I didn’t want to do anything because of the stigma attached.”
Stigma….. that’s been a battle for the Troops who find themselves having difficulty coping with day to day life, due to PTSD. For so many years, our Troops have been told to “suck it up” and led to believe that if they sought psychological help, that they would be ostracized by their peers, or in some way punished. That stigma is something that the Department of Defense and the branches of the Military are fighting hard to overcome. They’re working non-stop to let servicemembers know that it’s alright to ask for help and by doing so, it won’t mean the end of their career. One active duty soldier involved in the program went to Camp Zama, Japan following an especially tough tour for him in Baghdad. He says that he spiraled very quickly, began abusing alcohol and continually making mistakes.
“I just didn’t care anymore,” he said. “I had hit rock bottom and I didn’t like to think about what could have happened.”
http://soldiersmind.com/2007/08/21/pace-psychological-wounds-need-same-attention-as-physical-wounds/
“The program has done a lot for me and my family,” said a Marine veteran of the second battle for Fallujah. “I didn’t believe there was anything wrong with me when I came back to Kaneohe Baby. By the time I did, I didn’t want to do anything because of the stigma attached.”
Stigma….. that’s been a battle for the Troops who find themselves having difficulty coping with day to day life, due to PTSD. For so many years, our Troops have been told to “suck it up” and led to believe that if they sought psychological help, that they would be ostracized by their peers, or in some way punished. That stigma is something that the Department of Defense and the branches of the Military are fighting hard to overcome. They’re working non-stop to let servicemembers know that it’s alright to ask for help and by doing so, it won’t mean the end of their career. One active duty soldier involved in the program went to Camp Zama, Japan following an especially tough tour for him in Baghdad. He says that he spiraled very quickly, began abusing alcohol and continually making mistakes.
“I just didn’t care anymore,” he said. “I had hit rock bottom and I didn’t like to think about what could have happened.”
http://soldiersmind.com/2007/08/21/pace-psychological-wounds-need-same-attention-as-physical-wounds/
Posttraumatic Stress Disorder
What's in the future for PTSD?
What is so fascinating about PTSD is that it mirrors the diagnostic and treatment model (paradigm) we've come to know over the years as the Bio-Psycho-Social model. This model was first developed by Franz Alexander of Cedars-Sinai Medical Center and then elaborated on by George Engel (who coined the term) and John Romano at the University of Rochester.
In this model, there is a clear outside cause or external precipitating event, which is the Social part of the model. This event overwhelms our coping processes (mechanisms), which is the Psycho part of the model. These coping mechanisms are brought about (mediated) through the central nervous system (brain), particularly the autonomic nervous system and the HPA axis, which is the Bio part of the model. (The autonomic nervous system regulates the involuntary functions of the body, such as the producing and releasing of hormones by glands. The HPA axis refers to the brain's hypothalamus and the pituitary and adrenal glands.) As a matter of fact, we know that all of these systems interact in PTSD. Furthermore, there is a complex interplay between the different parts of the brain that regulate thoughts, memories, feelings, and behaviors, both healthy and diseased (pathological).
http://www.medicinenet.com/posttraumatic_stress_disorder/page7.htm
What is so fascinating about PTSD is that it mirrors the diagnostic and treatment model (paradigm) we've come to know over the years as the Bio-Psycho-Social model. This model was first developed by Franz Alexander of Cedars-Sinai Medical Center and then elaborated on by George Engel (who coined the term) and John Romano at the University of Rochester.
In this model, there is a clear outside cause or external precipitating event, which is the Social part of the model. This event overwhelms our coping processes (mechanisms), which is the Psycho part of the model. These coping mechanisms are brought about (mediated) through the central nervous system (brain), particularly the autonomic nervous system and the HPA axis, which is the Bio part of the model. (The autonomic nervous system regulates the involuntary functions of the body, such as the producing and releasing of hormones by glands. The HPA axis refers to the brain's hypothalamus and the pituitary and adrenal glands.) As a matter of fact, we know that all of these systems interact in PTSD. Furthermore, there is a complex interplay between the different parts of the brain that regulate thoughts, memories, feelings, and behaviors, both healthy and diseased (pathological).
http://www.medicinenet.com/posttraumatic_stress_disorder/page7.htm
Scientists Find PTSD Brain Molecule
A new study by scientists in the US has found a molecule in the brain of mice that when suppressed appears to make them forget the fear associated with a traumatic shock. It is hoped one day that this could lead to a drug to "cure" Post Traumatic Stress Disorder (PTSD).The study is published in the advanced online edition of the journal Nature Neuroscience and is the work of researchers from MIT's Picower Institute for Learning and Memory, based in Cambridge, Massachusetts.Led by Li-Huei Tsai, Picower Professor of Neuroscience at MIT, the scientists showed that inhibiting an enzyme called Cdk5 (a protein kinase) in the hippocampus, the centre in the brain that stores emotional memories, helps to extinguish fear learned in a particular context. But when Cdk5 activity is increased, the fear persists.PTSD results from an extreme stress reaction to an event that is perceived as highly threatening, where symptoms don't lessen with time, but remain for months and years afterwards, sometimes even getting worse. It is thought to arise from the brain's inability to extinguish the fear triggered by memories of the event. Symptoms of PTSD include flashbacks, overwhelming feelings of anger, anxiety and sometimes depression can follow too.Current psychological treatments for PTSD rely on learning to extinguish the fear triggered by memories of the trauma. This can be supported by drugs like antidepressants to help ease some of the symptoms, but there is currently no drug that addresses the underlying chemical processes directly, and they aren't well understood anyway, said the researchers. But, they said some research suggests that the mechanism that encodes memories of the trauma may also, in part, control their extinction.Tsai and colleagues already knew that Cdk5, when paired with another protein, p35, helps new neurons to grow and travel to their correct positions when the brain is developing. The aim of the current work with Cdk5 was to look into how the enzyme affected the formation and extinction of fear-related memories.They conducted an experiment where genetically engineered mice were given mild foot shocks in a certain environment. Then they put the mice in the same environment without giving them foot shocks and found that the mice with increased levels of Cdk5 continued to "freeze" with fear. But the mice in which the Cdk5 was inhibited were able to learn that they no longer needed to fear that environment any more. They were able to "let go" of the memory of the foot shock.Tsai said that:"Remarkably, inhibiting Cdk5 facilitated extinction of learned fear in mice. This data points to a promising therapeutic avenue to treat emotional disorders and raises hope for patients suffering from post-traumatic stress disorder or phobia."Explaining their findings, Tsai suggested that it could be because when Cdk5 is active, it prevents another key kinase from helping the extinction to take place.According to the National Center for PTSD in the US, 1 person out of every 12 experiences PTSD at some point in his or her life; this equates to over 5 million Americans living with PTSD at any one time. And a study by the US Army in 2004 showed that 1 in 8 soldiers returning from duty in Iraq had symptoms of PTSD. "A hippocampal Cdk5 pathway regulates extinction of contextual fear."Farahnaz Sananbenesi, Andre Fischer, Xinyu Wang, Christina Schrick, Rachael Neve, Jelena Radulovic and Li-Huei Tsai.Nature Neuroscience Published online: 15 July 2007doi:10.1038/nn1943Click here for Abstract.Click here for National Center for PTSD (US).Written by: Catharine PaddockWriter: Medical News Today Copyright: Medical News Today Not to be reproduced without permission of Medical News Today
http://www.medicalnewstoday.com/articles/76943.php
http://www.medicalnewstoday.com/articles/76943.php
Saturday, August 25, 2007
Relection and Presence
The Dialetic of Wakening
John Welwood
Professional Biography for John Welwood
John Welwood, Ph.D., is a clinical psychologist, psychotherapist, teacher, and author. He originally studied philosophy at Bowdoin College, and spent two years at the Sorbonne in Paris studying existentialist thought. As a graduate student he trained in existential psychology and worked closely with Eugene Gendlin at the University of Chicago, where he received his Ph.D. in clinical psychology in 1974. He has also been a practicing student of Buddhism and Eastern contemplative psychologies for thirty-five years. It is these two streams of influence that have shaped, in equal part, his innovative psycho spiritual approach. In the 1980s John Welwood emerged as a major figure in the leading-edge fields of transpersonal psychology and East/West psychology. The former Director of the East/West psychology program at the California Institute of Integral Studies in San Francisco, he is currently Associate Editor of the Journal of Transpersonal Psychology. He trains psychotherapists in "psychotherapy in a spiritual framework" and "the healing power of unconditional presence" and leads workshops on psychospiritual work and conscious relationship throughout the world.
I have come to a point in my healing journey where I see this study to be the truth for myself and I see myself changing from the abused victim to a thriver survivor.
John talks of a felt shift that is when movement in the body revealing a new sense of meaning and direction and the old fixation goes away.
He also speaks of satori which is a zen Buddhist meaning sudden awakening at the heart of zen.
He compared these two to see if they were the same thing or if they were different forms of ways to heal.
In his research as a psychotherapist he uncovered that the therapeutic process involved stepping back from one's felt experience in order to inquire into it in a dialogical manner. What he found to be different about the zen way of healing was that instead of stepping back and then looking at the trauma and having a felt shift like in psychotherapy that zen approached a more radical opening to whatever experience was at hand, instead of stepping back from it you directly recognize and meet ones experience as it is without concern for what it means where it comes from or where it leads. Zen believe this way you let go of the fixation on whatever arises in the mind and this eventually develops the capacity to relax and abide wakefully in the midst of whatever experience is arising. When there is no identification either with the observer or what is observed awareness remains undisturbed by any divisions and a new freedom, freshness, awareness, clarity and compassion become available.
I have seen this happening to me. I see from afar now instead of the experience up close and lets me evaluate what the reality of the situation is, taking apart layer by layer to reproduce a new understanding of the trauma I suffered and instead of internalizing it as in the past I have it now away from me reading it like a book so the logical part of my mind can develop whereas in survival mode it never developed grew due to only being able to focus on survival mode.
Part II Meditative Tradition of Tibetan Buddhism will continue in the next post.
You can go here and learn more of John Welwood.
http://www.johnwelwood.com/biography.htm
John Welwood
Professional Biography for John Welwood
John Welwood, Ph.D., is a clinical psychologist, psychotherapist, teacher, and author. He originally studied philosophy at Bowdoin College, and spent two years at the Sorbonne in Paris studying existentialist thought. As a graduate student he trained in existential psychology and worked closely with Eugene Gendlin at the University of Chicago, where he received his Ph.D. in clinical psychology in 1974. He has also been a practicing student of Buddhism and Eastern contemplative psychologies for thirty-five years. It is these two streams of influence that have shaped, in equal part, his innovative psycho spiritual approach. In the 1980s John Welwood emerged as a major figure in the leading-edge fields of transpersonal psychology and East/West psychology. The former Director of the East/West psychology program at the California Institute of Integral Studies in San Francisco, he is currently Associate Editor of the Journal of Transpersonal Psychology. He trains psychotherapists in "psychotherapy in a spiritual framework" and "the healing power of unconditional presence" and leads workshops on psychospiritual work and conscious relationship throughout the world.
I have come to a point in my healing journey where I see this study to be the truth for myself and I see myself changing from the abused victim to a thriver survivor.
John talks of a felt shift that is when movement in the body revealing a new sense of meaning and direction and the old fixation goes away.
He also speaks of satori which is a zen Buddhist meaning sudden awakening at the heart of zen.
He compared these two to see if they were the same thing or if they were different forms of ways to heal.
In his research as a psychotherapist he uncovered that the therapeutic process involved stepping back from one's felt experience in order to inquire into it in a dialogical manner. What he found to be different about the zen way of healing was that instead of stepping back and then looking at the trauma and having a felt shift like in psychotherapy that zen approached a more radical opening to whatever experience was at hand, instead of stepping back from it you directly recognize and meet ones experience as it is without concern for what it means where it comes from or where it leads. Zen believe this way you let go of the fixation on whatever arises in the mind and this eventually develops the capacity to relax and abide wakefully in the midst of whatever experience is arising. When there is no identification either with the observer or what is observed awareness remains undisturbed by any divisions and a new freedom, freshness, awareness, clarity and compassion become available.
I have seen this happening to me. I see from afar now instead of the experience up close and lets me evaluate what the reality of the situation is, taking apart layer by layer to reproduce a new understanding of the trauma I suffered and instead of internalizing it as in the past I have it now away from me reading it like a book so the logical part of my mind can develop whereas in survival mode it never developed grew due to only being able to focus on survival mode.
Part II Meditative Tradition of Tibetan Buddhism will continue in the next post.
You can go here and learn more of John Welwood.
http://www.johnwelwood.com/biography.htm
Friday, August 24, 2007



Tuesday, August 21, 2007
"Find Teresa Butler"
http://www.ipetitions.com/petition/findteresabutler?e
This is a girl from around the area I was raised in.
http://www.ipetitions.com/petition/findteresabutler?e
This is a girl from around the area I was raised in.
Fight for Justice
A tragedy can turn out to be to our greatest good, if it is approached and dealt with in a way that we can learn and grow. Personally, bringing awareness about sexual violence, my journey has shown me my personal spirit. It also has provided insight into the life as a survivor of sexual violence.I am truly blessed.Thank you to everyone at QuantumShift.tv , the 2007 Alberta International Victim Service Conference. Sincerely Holly Desimone
http://fightforjustice.blogspot.com/
http://fightforjustice.blogspot.com/
Self Defense Resource
In this issue of the SelfDefenseResource.com Newsletter:
1. Quick Tip: Use Any Object as a Weapon2. Technique: Dismount Assailant with Legs3. Virginia Tech Massacre4. New Articles5. Learn More: General Self-Defense
1. QUICK TIP: USE ANY OBJECT AS A WEAPON
Well, almost any everyday object can be used to protect yourself. Improvised weapons are everywhere around us.
When in Code Yellow, staying aware and scanning your environment for potential threats and escape routes, also identify anything that can be used as an improvised weapon.
It can be a stick, stone, or knife-like object that you can pick up and strike with. Shield-like objects to deflect a strike. Liquids and sprays to throw into a face. A structure that you can pull or push an assailant into.
http://www.selfdefenseresource.com/news/index.php
1. Quick Tip: Use Any Object as a Weapon2. Technique: Dismount Assailant with Legs3. Virginia Tech Massacre4. New Articles5. Learn More: General Self-Defense
1. QUICK TIP: USE ANY OBJECT AS A WEAPON
Well, almost any everyday object can be used to protect yourself. Improvised weapons are everywhere around us.
When in Code Yellow, staying aware and scanning your environment for potential threats and escape routes, also identify anything that can be used as an improvised weapon.
It can be a stick, stone, or knife-like object that you can pick up and strike with. Shield-like objects to deflect a strike. Liquids and sprays to throw into a face. A structure that you can pull or push an assailant into.
http://www.selfdefenseresource.com/news/index.php
The Last Straw
The Last Straw
Support, Motivation, Tips and Warning Signs of Domestic Violence
http://thelaststraw.wordpress.com/
Support, Motivation, Tips and Warning Signs of Domestic Violence
http://thelaststraw.wordpress.com/
Words express our emotion
FIVE FOR FIGHTING LYRICS"
World"
Got a package full of WishesA Time machine, a Magic WandA Globe made out of Gold No Instructions or CommandmentsLaws of Gravity orIndecisions to uphold Printed on the box I seeA.C.M.E.'s Build-a-World-to-beTake a chance - Grab a pieceHelp me to believe it What kind of world do you want?Think AnythingLet's start at the startBuild a masterpieceBe careful what you wish forHistory starts now... Should there be people or peoplesMoney, Funny pedestals for Fools who never payRaise your Army - Choose your SteepleDon't be shy, the satellites can look the other way Lose the Earthquakes - Keep the FaultsFill the oceans without the saltLet every Man own his own HandWhat kind of world do you wantThink AnythingLet's start at the startBuild a masterpieceBe careful what you wish forHistory starts now... Sunlight's on the BridgeSunlight's on the WayTomorrow's Calling There's more to this than LoveWhat Kind of world do you wantWhat Kind of world do you wantWhat Kind of world do you wantThink AnythingLet's start at the startBuild a masterpieceHistory Starts NowBe careful what you wish forStart Now
World"
Got a package full of WishesA Time machine, a Magic WandA Globe made out of Gold No Instructions or CommandmentsLaws of Gravity orIndecisions to uphold Printed on the box I seeA.C.M.E.'s Build-a-World-to-beTake a chance - Grab a pieceHelp me to believe it What kind of world do you want?Think AnythingLet's start at the startBuild a masterpieceBe careful what you wish forHistory starts now... Should there be people or peoplesMoney, Funny pedestals for Fools who never payRaise your Army - Choose your SteepleDon't be shy, the satellites can look the other way Lose the Earthquakes - Keep the FaultsFill the oceans without the saltLet every Man own his own HandWhat kind of world do you wantThink AnythingLet's start at the startBuild a masterpieceBe careful what you wish forHistory starts now... Sunlight's on the BridgeSunlight's on the WayTomorrow's Calling There's more to this than LoveWhat Kind of world do you wantWhat Kind of world do you wantWhat Kind of world do you wantThink AnythingLet's start at the startBuild a masterpieceHistory Starts NowBe careful what you wish forStart Now
Sunday, August 19, 2007
The Drive behind a Traumatized Mind Part 2 "
Continuing on now with the fear/independence issue. How is fear and Independence related?
The amygdala itself is a highly complex collection of nuclei, so it could conceivably support different emotions in different areas -- as it does appear to do in the case of fear & anger
Fear--to be afraid of
Independent--(1) : not subject to control by others
From Merriam-Webster online: http://www.m-w.com/cgi-bin/dictionary
The feeling of being afraid to complete something, to fail, to be looked down upon. Have you ever had these feelings?
The feeling of not being controlled by someone whether they are present or not? I will persist until it gets done and cant look beyond to see if it might hurt me or put me in danger or foresight into maybe there is a different angle to what is perceived. Somewhat like fear and independence are instruments of the animal instinct whereas you have to survive. I don't want to veer to far off onto this road because you can go far with the information, so lets just equal it to fear=confidence=a part of animal instincts. What we have is this::
The central nucleus mediates expression of conditioned fear responses. The "defensive response" to a threatening stimulus consists of elevated heart rate (mediated by the lateral hypothalamus) and a "freeze state" (mediated by the central gray), both of which receive input from the central nucleus of the amygdala. Lesions to the lateral hypothalamus eliminate the effect on heart rate, but not the "freeze state", whereas lesions to the central gray have the opposite effect. Both responses can be evoked by amygdala stimulation. The bed nucleus of the stria terminalis mediates the release of pituitary-adrenal stress hormone (Corticotropin-Releasing Hormone, CRH) in response to fear. CRH causes the adrenal gland to release epinephrine & cortisol. Chronic stress causes cortisol-induced release of epinephrine from the locus coeruleus to the amygdala -- creating a vicious cycle.
Now I will continue with the car incident, I worked for days upon days almost eight in fact, never giving relenting only this raw need to complete with no foresee into any other avenue. No insight into danger of any kind my only concern was of failing my family by not getting the car fixed. I felt fear of both failure and 100% independent cant ask for help. What stopped me from getting help, I would have to rely on someone else, the control would be in their corner and I would have no input as to whether the out outcome would be good or bad. My brain reflectively thought negative so the only thing flowing at first was negativity. So my statement at the beginning of this post was, Why is Independence so important to a traumatized mind? Its a controlled reaction our amygdala gets juiced up on sensors whereas in a non traumatized amygdala once the fear stage is proven to not be there then the sensors go back to normal flow, in a traumatized mind though we never make it to the reset phase.
Connections
The amygdalae send impulses to the hypothalamus for important activation of the sympathetic nervous system, to the reticular nucleus for increased reflexes, to the nuclei of the trigeminal nerve and facial nerve for facial expressions of fear, and to the ventral tegmental area, locus coeruleus, and laterodorsal tegmental nucleus for activation of dopamine, norepinephrine and epinephrine.[4]
The cortical nucleus is involved in the sense of smell and pheromone-processing. It receives input from the olfactory bulb and olfactory cortex. The lateral amygdalae, which send impulses to the rest of the basolateral complexes and to the centromedial nuclei, receive input from the sensory systems. The centromedial nuclei are the main outputs for the basolateral complexes, and are involved in emotional arousal in rats and cats.[4][5]
http://en.wikipedia.org/wiki/Amygdala
Let me break it down a little more unscientifically blood flow is restricted to that area of the brain known as the amygdala and thus it does not get what is needed so it doesnt grow.
As this primary sensory input arrives, it is matched against previously stored patterns of activation. If the pattern is unknown, or is associated with previous threat, the brain will activate a set of responses that are designed to help promote survival. (This alarm response is at the heart of the post-traumatic symptoms seen in so many maltreated children.)
http://www.childtraumaacademy.com/amazing_brain/lesson01/page03.html
So from stored patterns our brain pulls the fear alarm but then the reset button cant be found, so what is the drive behind independence simply put stored patterns from our image files. How can we put new images in and expand our amygdala?(that will be the next part we discuss.)
So when you feel your threat level raised what can you do so you dont go full blown fear driven so you can overcome and not get stuck in the cycle of of past patterns?
This is what I did maybe it can help you. Remembering I am only human if this triggers things and feelings in you reach out to someone for professional help. I had to sit with myself only after getting sick from working on the car. I never truly saw it coming and when it hit I had no idea what had happened, I could make up an excuse for the pain, Oh I pulled to hard, I pushed to hard suck it up, you cant be beat by this......what I had done was ignore the part flaring up so that part stayed in the fear independent mode. My focus was so intense it paralized what I have learned and that was to slow my mind down enough to refocus my focus and see why the fear is active and does it need to be. Sounds simple let me tell you it is not but change can happen new images can implode the old. Meditation works for me psycho therapy works for me find your voice change your amygdala change the patterns you see.
A very good read http://ldc.upenn.edu/myl/llog/KillgoreAmygdala.pdf
One more thing then we will put to close enough information to let sink in. Now for the fourth part of the outline is amydgala can you increase yours?
It seems science has given us a chance to try lets take a look at it. You can try it here is a website with instructions just takes your time.
http://www.viewzone.com/amygdala/index3.html
Focus on the best time you have ever had in your life the got it, now hold that memory for thirty seconds. A researcher named TDA Lingo pinpointed this area of the brain (amygdala) that is the button to push for when you know which one you can self stimulate your brain and increase it. Lingo studied 309 students shen the study was finished the findings were tremendous on the Getezels, Jackson Creativity Index that is imagination was increased between 500 to 1400 %. Back to the best time you have ever had in your life congratulations you have just tickled the amygdala and stimulated growth. I hope you will find a piece of knowledge in this article to take for yourself by stimulating our world one thought at a time we can undo some of the things we have innocently had to struggle through.
http://www.viewzone.com/amygdala/index4.html
http://ldc.upenn.edu/myl/llog/KillgoreAmygdala.pdf
Saturday, August 18, 2007
"The Drive behind a Traumatized Mind
Why is Independence so important to a traumatized mind? I have done a lot of research on this issue, as I encountered it's impact this last month. So why does the traumatized mind react to self independence and not able to rely on others for help. Ok lets break this down a bit,
1. Brain part that plays key function in independence.
2. Why does our brain alter and how?
3. What are some signs and how can you control them?
4. Amygdala can you increase yours
Brain part that plays key function in independence.
The Amygdala is the part we are going to focus on.
Amygdala
AMYGDALA ANATOMY
The amygdala in a human is not much bigger than an almond (the Greek root word). At the base of the brain, the elevation of the parahippocampus at the uncus is due to the amygdala, which lies beneath it. The amygdala is really three collections of nuclei. The largest (and best differentiated) portion of the amygdaloid complex is the basolateral nuclear group [BL], consisting of the lateral nucleus, the multi-faceted basal nucleus and the accessory basal nucleus. The other major portion consists of the centromedial group [Ce-M], consisting of the central nucleus and the medial nucleus. The Ce-M group is connected through a strand of fibers (the stria terminalis) -- traveling alongside the tail of the caudate nucleus) to an area by the hypothalamus known as the bed nucleus of the stria terminalis [BST]. Cell types in the BST are identical to those in the Ce-M, causing the BST to be included in the definition of the "extended amygdala". The BST lies in the basal forebrain (substantia innominata), which also contains the nucleus accumbens, the basal nucleus of Meynert and the ventral portions of the putamen and globus pallidus (which are basal ganglia). The smallest portion of the amygdaloid complex is the cortical nucleus, also known as the olfactory amygdala because the primary input to the cortical nuclear group is from the olfactory bulb and olfactory cortex. (The naming and groupings of nuclei in the amygdala is far from standard, which can make the literature on the subject unnecessarily difficult to understand. Some authors group the cortical and centromedial nuclei together as the cortiomedial amygdala.)
Why does our brain alter and why?
Two major bundles of fibers connect the amygdala with other areas of the brain: the stria terminalis and the ventral amygdalofugal pathway. The centromedial amygdala projects through the stria terminalis primarily to the hypothalamus and through the ventral amygdalofugal tract to the brain stem, where it can influence hormonal and somatomotor aspects of behavior & emotional states (eg, eating, drinking & sex).
Monkeys without amygdalas have difficulty learning to associate a light-signal with an electric shock -- and also have difficulty associating a neutral stimulus with a food reward. It has been suggested that the amygdala functions to associate sensation with reward or punishment. Amphetamine injections to the ventral striatum enhance the effects of a conditioned reinforcing stimulus only if the amygdala is intact.
Neurons in the lateral, basal and central nuclei of primate amygdalas have been found to respond to visual stimuli associated with a food reward. But when the reward was changed to an aversive food (saline) the response of these neurons did not change -- in contrast to neurons in the orbitofrontal cortex and basal forebrain which show a rapid reversal in response to a positive reinforcement becoming a negative one. This implies that the amygdala neuron response corresponds to whether a stimulus has reward/punishment significance (and merits attention), rather than associating the stimulus with a reward or punishment.
Signals from the thalamus, co-ordinated with signals from the visual cortex, evidently allow the amygdala to assist in focusing attention in response to fear [SCIENCE 300:568-569 (2003)]. Fearful images -- notably other humans with fearful facial expressions -- apparently increase attention, arousal and cortical processing through amygdala mediation.
LTP (Long-Term Potentiation) can occur in amygdala brain slices. The basal nucleus has high levels of NMDA receptors. Infusion of NMDA antagonists into the amygdala blocks the acquisition, but not the expression, of conditioned fear. However, infusion of NMDA has no effect on the acquisition of conditioned taste aversion. Lesions or electrical stimulation of the amygdala impair aversion taste learning without affecting maze learning (which is dependent on the hippocampus). Conversely, lesions or electrical stimulation of the hippocampus impairs maze learning, but not taste aversion learning. Human patients with amygdala lesions show impaired immediate visual recognition, while visual memory is normal.
Like the hippocampus, the amygdala is rich in receptors for cortisol (hydrocortisone, ie, stress hormone). While prolonged stress (prolonged cortisol exposure) impairs LTP in the hippocampus, the same stresses facilitate LTP in the amygdala [NEUROCHEMICAL RESEARCH 28(1):1735-1742 (2003)].
Both the hippocampus and the amygdala (particularly the lateral nucleus) contain high concentrations of receptors for the benzodiazepine anti-anxiety drugs. Microinjections of benzodiazepines into the amygdala reduces fear & anxiety, but this effect is not seen upon microinjection into the hippocampus. Humans with amygdala lesions show a decrease in "emotional tension". It has been postulated that benzodiazepines may act on the lateral nucleus to prevent the linkage of emotional significance to sensory stimuli -- prior to conscious processing.
I know this is a lot of reading but we have to understand what ticks to understand why we have the reactions we do.
AS you can see the amygdala plays a key function in our emotional side of the brain (right side). The fear releasing hormone cortisol can take the pathways and reroute them when the fear releasing hormones are released in high levels or stay in the state of fear for long periods of time. Therefore it starts rewiring our brain and functions, now getting to the independence factor. Most traumatized child brains are stuck in routes of survivial or fear mode. So we continue to stay in that rut and when dealt fear we respond to a differently wired brain and reactions.
My example;
For the last month our car has been broken down. It was something that look doable without much confusion. My son and I started working on it and it was in worse condition than we thought. For two weeks I sprayed all kinds of rusting chemicals on it torqued so hard I thougth I had brusied a rib, but I wouldnt give up, I never thought of getting someone else to help. I had one thought I will not let this beat me, I cannot fail at this!! Have you have had that feeling when you were kinda in over your head but what tool did you use. This is where the fear independence factor comes in.
OK I will let you take this part in and later this afternoon we will continue. Once we trace where are brains got rewired there are ways to undo some of the growth problems.
http://www.benbest.com/science/anatmind/anatmd9.html
1. Brain part that plays key function in independence.
2. Why does our brain alter and how?
3. What are some signs and how can you control them?
4. Amygdala can you increase yours
Brain part that plays key function in independence.
The Amygdala is the part we are going to focus on.
Amygdala
AMYGDALA ANATOMY
The amygdala in a human is not much bigger than an almond (the Greek root word). At the base of the brain, the elevation of the parahippocampus at the uncus is due to the amygdala, which lies beneath it. The amygdala is really three collections of nuclei. The largest (and best differentiated) portion of the amygdaloid complex is the basolateral nuclear group [BL], consisting of the lateral nucleus, the multi-faceted basal nucleus and the accessory basal nucleus. The other major portion consists of the centromedial group [Ce-M], consisting of the central nucleus and the medial nucleus. The Ce-M group is connected through a strand of fibers (the stria terminalis) -- traveling alongside the tail of the caudate nucleus) to an area by the hypothalamus known as the bed nucleus of the stria terminalis [BST]. Cell types in the BST are identical to those in the Ce-M, causing the BST to be included in the definition of the "extended amygdala". The BST lies in the basal forebrain (substantia innominata), which also contains the nucleus accumbens, the basal nucleus of Meynert and the ventral portions of the putamen and globus pallidus (which are basal ganglia). The smallest portion of the amygdaloid complex is the cortical nucleus, also known as the olfactory amygdala because the primary input to the cortical nuclear group is from the olfactory bulb and olfactory cortex. (The naming and groupings of nuclei in the amygdala is far from standard, which can make the literature on the subject unnecessarily difficult to understand. Some authors group the cortical and centromedial nuclei together as the cortiomedial amygdala.)
Why does our brain alter and why?
Two major bundles of fibers connect the amygdala with other areas of the brain: the stria terminalis and the ventral amygdalofugal pathway. The centromedial amygdala projects through the stria terminalis primarily to the hypothalamus and through the ventral amygdalofugal tract to the brain stem, where it can influence hormonal and somatomotor aspects of behavior & emotional states (eg, eating, drinking & sex).
Monkeys without amygdalas have difficulty learning to associate a light-signal with an electric shock -- and also have difficulty associating a neutral stimulus with a food reward. It has been suggested that the amygdala functions to associate sensation with reward or punishment. Amphetamine injections to the ventral striatum enhance the effects of a conditioned reinforcing stimulus only if the amygdala is intact.
Neurons in the lateral, basal and central nuclei of primate amygdalas have been found to respond to visual stimuli associated with a food reward. But when the reward was changed to an aversive food (saline) the response of these neurons did not change -- in contrast to neurons in the orbitofrontal cortex and basal forebrain which show a rapid reversal in response to a positive reinforcement becoming a negative one. This implies that the amygdala neuron response corresponds to whether a stimulus has reward/punishment significance (and merits attention), rather than associating the stimulus with a reward or punishment.
Signals from the thalamus, co-ordinated with signals from the visual cortex, evidently allow the amygdala to assist in focusing attention in response to fear [SCIENCE 300:568-569 (2003)]. Fearful images -- notably other humans with fearful facial expressions -- apparently increase attention, arousal and cortical processing through amygdala mediation.
LTP (Long-Term Potentiation) can occur in amygdala brain slices. The basal nucleus has high levels of NMDA receptors. Infusion of NMDA antagonists into the amygdala blocks the acquisition, but not the expression, of conditioned fear. However, infusion of NMDA has no effect on the acquisition of conditioned taste aversion. Lesions or electrical stimulation of the amygdala impair aversion taste learning without affecting maze learning (which is dependent on the hippocampus). Conversely, lesions or electrical stimulation of the hippocampus impairs maze learning, but not taste aversion learning. Human patients with amygdala lesions show impaired immediate visual recognition, while visual memory is normal.
Like the hippocampus, the amygdala is rich in receptors for cortisol (hydrocortisone, ie, stress hormone). While prolonged stress (prolonged cortisol exposure) impairs LTP in the hippocampus, the same stresses facilitate LTP in the amygdala [NEUROCHEMICAL RESEARCH 28(1):1735-1742 (2003)].
Both the hippocampus and the amygdala (particularly the lateral nucleus) contain high concentrations of receptors for the benzodiazepine anti-anxiety drugs. Microinjections of benzodiazepines into the amygdala reduces fear & anxiety, but this effect is not seen upon microinjection into the hippocampus. Humans with amygdala lesions show a decrease in "emotional tension". It has been postulated that benzodiazepines may act on the lateral nucleus to prevent the linkage of emotional significance to sensory stimuli -- prior to conscious processing.
I know this is a lot of reading but we have to understand what ticks to understand why we have the reactions we do.
AS you can see the amygdala plays a key function in our emotional side of the brain (right side). The fear releasing hormone cortisol can take the pathways and reroute them when the fear releasing hormones are released in high levels or stay in the state of fear for long periods of time. Therefore it starts rewiring our brain and functions, now getting to the independence factor. Most traumatized child brains are stuck in routes of survivial or fear mode. So we continue to stay in that rut and when dealt fear we respond to a differently wired brain and reactions.
My example;
For the last month our car has been broken down. It was something that look doable without much confusion. My son and I started working on it and it was in worse condition than we thought. For two weeks I sprayed all kinds of rusting chemicals on it torqued so hard I thougth I had brusied a rib, but I wouldnt give up, I never thought of getting someone else to help. I had one thought I will not let this beat me, I cannot fail at this!! Have you have had that feeling when you were kinda in over your head but what tool did you use. This is where the fear independence factor comes in.
OK I will let you take this part in and later this afternoon we will continue. Once we trace where are brains got rewired there are ways to undo some of the growth problems.
http://www.benbest.com/science/anatmind/anatmd9.html
Thursday, August 16, 2007
Update on posts
Thank you all for hanging with me there will lots of post this weekend I have been sick so hang with me, I have a huge post coming this weekend on Survivors and a true story so see ya this weekend.
Kathy
Kathy
Tuesday, August 14, 2007
A simple thought process can be a gateway for the Amygdala
By deliberately focusing mental energy and activity- a simple thought process- on the anterior amygdala, this causes an increase in frontal lobes processes, which instantly causes increased and measurable levels of intelligence, creativity, pleasure, and often various "normal-paranormal" experiences. The method can be as simple as "imaging" a feather tickling the amygdala, which automatically shunts neurochemical activity forward into the previously "dormant" frontal lobes. The amygdala can be seen as a gateway click switch, somewhat like the light switch on your wall. But in your brain, you "click" on the big light bulb in your frontal lobes.
Russian neurosurgeon Alexandre Luria, along with many other distinguished researchers have repeatedly shown us that the frontal lobes are at least 90% dormant, "untapped", unused. Although some may object to this description of the brain, it is one effective way of describing the infinite potential of the human brain. We normally don't live up to even a fraction of what is available or possible. It is the great cosmic joke.
Self-amygdala stimulation without electrodes can be performed by using the brain's capacity for guided imagery.
http://www.viewzone.com/amygdala/index3.html
Russian neurosurgeon Alexandre Luria, along with many other distinguished researchers have repeatedly shown us that the frontal lobes are at least 90% dormant, "untapped", unused. Although some may object to this description of the brain, it is one effective way of describing the infinite potential of the human brain. We normally don't live up to even a fraction of what is available or possible. It is the great cosmic joke.
Self-amygdala stimulation without electrodes can be performed by using the brain's capacity for guided imagery.
http://www.viewzone.com/amygdala/index3.html
Popping Your Frontals
New research in the field of brain and behavior now allows any ordinary person to learn how to control and self-stimulate their own brain for such results as mentioned above. Studies by one particular behaviorist and researcher, T.D.A. Lingo, in his work from 1957 through 1993, has been able to pinpoint this area of the brain which seems to be responsible for releasing enormous levels of untapped intelligence, creativity and pleasure. Additionally, and remarkably so, self-amygdala stimulation frequently additionally turns on such "hidden" brain functions as pre-cognition, clairvoyance, clairaudience, telepathy, telekinesis, and in can even allow the ability for some individuals the ability to communicate with non-ordinary physical and non-physical intelligences and entities.
http://www.viewzone.com/amygdala/index2.html
http://www.viewzone.com/amygdala/index2.html
Amygdala can you increase yours?
I want you to think of the best time you have ever had in your life........Got it?
Now, multiply that experience, that feeling, times ten. Multiply it times a hundred, or a thousand. Or ten thousand. Or even more.
You can turn on increased creativity, intelligence, pleasure, even ESP and other paranormal abilities as easily as clicking on a light switch. You can have "the best day of your life" over and over, each time better than the last. You may even be able to move clouds and change the weather using the incredible power of your own human infinity machine- your brain.
That is exactly what you will experience- no exaggeration in the least- when you learn how to self-stimulate a part of your brain know as the amygdala. This is not wishful thinking or new-age hocus-pocus. This is what the latest brain and behavior research is now showing us is possible........for anyone. The method for amygdala self-stimulation is easy, and has been learned by persons ages 6 to 86. The basic method can be learned and taught by anyone, for free. It is democratic in the extreme. You are getting started by reading this article. Results are often immediate, and are accumulative- it gets better the more you do it. Unlike stage magic, this is no illusion. This is real brain magic.
http://www.viewzone.com/amygdala/index.html
Now, multiply that experience, that feeling, times ten. Multiply it times a hundred, or a thousand. Or ten thousand. Or even more.
You can turn on increased creativity, intelligence, pleasure, even ESP and other paranormal abilities as easily as clicking on a light switch. You can have "the best day of your life" over and over, each time better than the last. You may even be able to move clouds and change the weather using the incredible power of your own human infinity machine- your brain.
That is exactly what you will experience- no exaggeration in the least- when you learn how to self-stimulate a part of your brain know as the amygdala. This is not wishful thinking or new-age hocus-pocus. This is what the latest brain and behavior research is now showing us is possible........for anyone. The method for amygdala self-stimulation is easy, and has been learned by persons ages 6 to 86. The basic method can be learned and taught by anyone, for free. It is democratic in the extreme. You are getting started by reading this article. Results are often immediate, and are accumulative- it gets better the more you do it. Unlike stage magic, this is no illusion. This is real brain magic.
http://www.viewzone.com/amygdala/index.html
INDICATIONS OF AMYGDALA FUNCTION
This is a very indepth reading but taking a bit apart makes us understand some of the main actions and what leads to our emotional response verus logical response.
Monkeys without amygdalas have difficulty learning to associate a light-signal with an electric shock -- and also have difficulty associating a neutral stimulus with a food reward. It has been suggested that the amygdala functions to associate sensation with reward or punishment. Amphetamine injections to the ventral striatum enhance the effects of a conditioned reinforcing stimulus only if the amygdala is intact.
Neurons in the lateral, basal and central nuclei of primate amygdalas have been found to respond to visual stimuli associated with a food reward. But when the reward was changed to an aversive food (saline) the response of these neurons did not change -- in contrast to neurons in the orbitofrontal cortex and basal forebrain which show a rapid reversal in response to a positive reinforcement becoming a negative one. This implies that the amygdala neuron response corresponds to whether a stimulus has reward/punishment significance (and merits attention), rather than associating the stimulus with a reward or punishment.
Signals from the thalamus, co-ordinated with signals from the visual cortex, evidently allow the amygdala to assist in focusing attention in response to fear [SCIENCE 300:568-569 (2003)]. Fearful images -- notably other humans with fearful facial expressions -- apparently increase attention, arousal and cortical processing through amygdala mediation.
http://www.benbest.com/science/anatmind/anatmd9.html
Monkeys without amygdalas have difficulty learning to associate a light-signal with an electric shock -- and also have difficulty associating a neutral stimulus with a food reward. It has been suggested that the amygdala functions to associate sensation with reward or punishment. Amphetamine injections to the ventral striatum enhance the effects of a conditioned reinforcing stimulus only if the amygdala is intact.
Neurons in the lateral, basal and central nuclei of primate amygdalas have been found to respond to visual stimuli associated with a food reward. But when the reward was changed to an aversive food (saline) the response of these neurons did not change -- in contrast to neurons in the orbitofrontal cortex and basal forebrain which show a rapid reversal in response to a positive reinforcement becoming a negative one. This implies that the amygdala neuron response corresponds to whether a stimulus has reward/punishment significance (and merits attention), rather than associating the stimulus with a reward or punishment.
Signals from the thalamus, co-ordinated with signals from the visual cortex, evidently allow the amygdala to assist in focusing attention in response to fear [SCIENCE 300:568-569 (2003)]. Fearful images -- notably other humans with fearful facial expressions -- apparently increase attention, arousal and cortical processing through amygdala mediation.
http://www.benbest.com/science/anatmind/anatmd9.html
Monday, August 13, 2007
STILL STAGGERING FROM THE BLOW Living with a Trauma
There's no single description for what life is like for all individuals with PTSD. Because of the many possible levels of traumatization, the symptoms vary considerably. For some, life becomes a boring, meaningless pursuit, with no emotional ups and downs, nothing to get excited about. For others, it is a perpetual struggle, and threats are everywhere. They are constantly uptight and on their guard, anticipating trouble at times when others would be relaxed. For still others, life becomes a big drag; they're depressed, and they slog through their days isolated from the rest of the world.
But despite all the differences, certain common themes weave through the experience of everyone who has a trauma disorder. If you or a loved one has been traumatized, you should be able to recognize these themes.
When a traumatization persists for more than a few weeks, it begins to become a whole way of life, and everything that matters to you is affected. It's not just the intrusive thoughts, it's the life you're leading as well, particularly the way you feel about yourself and where you belong in the world of people. The effects of the trauma itself—what I call the initial trauma—can be viewed separately from the changes in your relationships with other people (the relational trauma). Initial trauma refers to the direct effects of the trauma on your thoughts and emotions—the reexperiencing, the avoidance/emotional numbing, and the hyperarousal. Relational trauma refers to the changes in your relationships and the way in which you view yourself, which is influenced by your relationships. This disruption of your social world is reflected in your symptoms of alienation and your difficulty with relationships. Let's look at one of the examples from Chapter 1 in order to get a feel for the basic difference between the symptoms of the initial and relational traumas.
http://www.emotionalsafety.net/brink/2.htm
But despite all the differences, certain common themes weave through the experience of everyone who has a trauma disorder. If you or a loved one has been traumatized, you should be able to recognize these themes.
When a traumatization persists for more than a few weeks, it begins to become a whole way of life, and everything that matters to you is affected. It's not just the intrusive thoughts, it's the life you're leading as well, particularly the way you feel about yourself and where you belong in the world of people. The effects of the trauma itself—what I call the initial trauma—can be viewed separately from the changes in your relationships with other people (the relational trauma). Initial trauma refers to the direct effects of the trauma on your thoughts and emotions—the reexperiencing, the avoidance/emotional numbing, and the hyperarousal. Relational trauma refers to the changes in your relationships and the way in which you view yourself, which is influenced by your relationships. This disruption of your social world is reflected in your symptoms of alienation and your difficulty with relationships. Let's look at one of the examples from Chapter 1 in order to get a feel for the basic difference between the symptoms of the initial and relational traumas.
http://www.emotionalsafety.net/brink/2.htm
Sunday, August 12, 2007
Veterans seeking treatment for posttraumatic stress disorder: What about comorbid chronic pain?
Compare non war PTSD and war PTSD read below on war ptsd and see how you compare if you have trauma in your life.
Given that high rates of comorbid chronic pain diagnoses are likely in PTSD treatment-seeking veterans, considering how this might influence treatment planning becomes salient. Studies suggest that the comorbidity of PTSD and pain may profoundly affect psychosocial and physical functioning as well as quality of life [51-54]. From a theoretical perspective, the concept of "mutual maintenance" of pain and PTSD becomes important to consider [45,48]. Similar to the theory of shared vulnerability, the mutual maintenance hypothesis proposes that the cognitive, affective, psychophysiological, and behavioral symptoms of both disorders react in synergistic ways. For example, a patient with PTSD who develops a back problem may overreact to the painful stimuli (e.g., as though it were life-threatening). Thus, the patient becomes more likely to avoid any situation that he or she believes may trigger pain in addition to the situations he or she avoids for fear of triggering memories of the trauma. The result of this cycle of avoidance is increased restriction and disability. Fortunately, cognitive-behavioral treatment programs that emphasize the importance of exposures to feared situations in a safe and controlled manner are recommended for both PTSD and chronic pain problems [55-56]. Further, these treatment programs address underlying maladaptive cognitions (e.g., belief that back pain is life-threatening) through cognitive restructuring. Given that cognitive behavioral interventions are empirically supported for the treatment of both PTSD and chronic pain and that these programs may target mutually maintaining factors (e.g., avoidance behavior), examining the effect of PTSD treatment on chronic pain is important.
Unfortunately, very few PTSD treatment studies have also directly examined the effect of the treatment on pain problems and most are case studies. A study of three patients with both pain and PTSD revealed that while pain treatment was not effective, PTSD treatment was useful [29]. Similarly, in a small study of headache patients, no improvement was shown until the PTSD symptoms were addressed in patients with both headaches and PTSD [57]. In contrast, at a recent case conference, experts discussed a single patient with pain and PTSD for whom PTSD treatment was not effective [58-59], although leaders in the field had all recommended this approach [60-62]. Shipherd and colleagues investigated the effect of PTSD treatment on chronic pain with a sample of six women with chronic pain and PTSD after car accidents [63]. These women received 12 weeks of manualized cognitive behavioral PTSD treatment that explicitly avoided discussion of pain-related issues. Results indicated a decrease in PTSD symptoms as well as in other psychiatric symptoms for most patients. Although subjective pain ratings did not change posttreatment, pain-related functional improvements were noted, including a return to full-time work for the majority of participants. These results suggest that the benefits of PTSD treatment may generalize to comorbid chronic pain problems. However, importantly, the treatment took place in a carefully controlled research context that may or may not be applicable to naturally occurring treatment venues [64]. The studies conducted to date on the effects of PTSD treatment on comorbid chronic pain complaints have all been small sample studies with some promising results. However, large-scale controlled studies of the effects of PTSD treatment on pain have not yet been published. Another limitation of the existing literature is that the treatments have been conducted in small controlled trials, in spite of the availability of large databases of naturally collected data from PTSD treatment (e.g., VA databases) that have yet to be fully explored in this regard. The current study is one attempt to use this preexisting data to better understand the prevalence of chronic pain problems in patients with PTSD and to explore whether any changes occur in pain ratings before, during, or after PTSD treatment.
http://www.rehab.research.va.gov/jour/2/shipherd.html07/44/
Given that high rates of comorbid chronic pain diagnoses are likely in PTSD treatment-seeking veterans, considering how this might influence treatment planning becomes salient. Studies suggest that the comorbidity of PTSD and pain may profoundly affect psychosocial and physical functioning as well as quality of life [51-54]. From a theoretical perspective, the concept of "mutual maintenance" of pain and PTSD becomes important to consider [45,48]. Similar to the theory of shared vulnerability, the mutual maintenance hypothesis proposes that the cognitive, affective, psychophysiological, and behavioral symptoms of both disorders react in synergistic ways. For example, a patient with PTSD who develops a back problem may overreact to the painful stimuli (e.g., as though it were life-threatening). Thus, the patient becomes more likely to avoid any situation that he or she believes may trigger pain in addition to the situations he or she avoids for fear of triggering memories of the trauma. The result of this cycle of avoidance is increased restriction and disability. Fortunately, cognitive-behavioral treatment programs that emphasize the importance of exposures to feared situations in a safe and controlled manner are recommended for both PTSD and chronic pain problems [55-56]. Further, these treatment programs address underlying maladaptive cognitions (e.g., belief that back pain is life-threatening) through cognitive restructuring. Given that cognitive behavioral interventions are empirically supported for the treatment of both PTSD and chronic pain and that these programs may target mutually maintaining factors (e.g., avoidance behavior), examining the effect of PTSD treatment on chronic pain is important.
Unfortunately, very few PTSD treatment studies have also directly examined the effect of the treatment on pain problems and most are case studies. A study of three patients with both pain and PTSD revealed that while pain treatment was not effective, PTSD treatment was useful [29]. Similarly, in a small study of headache patients, no improvement was shown until the PTSD symptoms were addressed in patients with both headaches and PTSD [57]. In contrast, at a recent case conference, experts discussed a single patient with pain and PTSD for whom PTSD treatment was not effective [58-59], although leaders in the field had all recommended this approach [60-62]. Shipherd and colleagues investigated the effect of PTSD treatment on chronic pain with a sample of six women with chronic pain and PTSD after car accidents [63]. These women received 12 weeks of manualized cognitive behavioral PTSD treatment that explicitly avoided discussion of pain-related issues. Results indicated a decrease in PTSD symptoms as well as in other psychiatric symptoms for most patients. Although subjective pain ratings did not change posttreatment, pain-related functional improvements were noted, including a return to full-time work for the majority of participants. These results suggest that the benefits of PTSD treatment may generalize to comorbid chronic pain problems. However, importantly, the treatment took place in a carefully controlled research context that may or may not be applicable to naturally occurring treatment venues [64]. The studies conducted to date on the effects of PTSD treatment on comorbid chronic pain complaints have all been small sample studies with some promising results. However, large-scale controlled studies of the effects of PTSD treatment on pain have not yet been published. Another limitation of the existing literature is that the treatments have been conducted in small controlled trials, in spite of the availability of large databases of naturally collected data from PTSD treatment (e.g., VA databases) that have yet to be fully explored in this regard. The current study is one attempt to use this preexisting data to better understand the prevalence of chronic pain problems in patients with PTSD and to explore whether any changes occur in pain ratings before, during, or after PTSD treatment.
http://www.rehab.research.va.gov/jour/2/shipherd.html07/44/
Saturday, August 11, 2007
Size of brain structure could signal vulnerability to anxiety disorders
Area appears smaller in those that continue to react to images associated with discomfort
Individuals respond with physical and emotional distress to situations that recall traumatic memories. Such responses usually diminish gradually, as those situations are repeated without unpleasant occurrences; this is called "extinction memory." But some people continue to respond fearfully and develop post-traumatic stress disorder (PTSD).
http://www.researchmatters.harvard.edu/story.php?article_id=904
Individuals respond with physical and emotional distress to situations that recall traumatic memories. Such responses usually diminish gradually, as those situations are repeated without unpleasant occurrences; this is called "extinction memory." But some people continue to respond fearfully and develop post-traumatic stress disorder (PTSD).
http://www.researchmatters.harvard.edu/story.php?article_id=904
Decoding the babel of brain cells
They contain the recipe for movement
If brain cell messages could be separated from the "noise" of other brain activity and clearly understood, researchers would be closer to repairing damage caused by a number of nervous system diseases paralyzing injuries and combat wounds.
http://www.researchmatters.harvard.edu/story.php?article_id=813
If brain cell messages could be separated from the "noise" of other brain activity and clearly understood, researchers would be closer to repairing damage caused by a number of nervous system diseases paralyzing injuries and combat wounds.
http://www.researchmatters.harvard.edu/story.php?article_id=813
Traumatic Epilepsy Centers Proposed For Returning Vets
U.S. Senators Patty Murray (D-Wash.) and Larry Craig (R-ID) introduced joint legislation to establish six Department of Veterans Affairs (VA) Epilepsy Centers of Excellence across the country. The bill is designed to with the treatment of post traumatic epilepsy following brain trauma.
The Murray-Craig bill authorizes $6 million annually for the Epilepsy Centers of Excellence to support clinical, research and education efforts surrounding the incidence of epilepsy among current and future veterans with head and brain injuries.
According to Senator Craig, "Experts have indicated that half of all Vietnam veterans who suffered penetrating brain injuries suffer from what is known as 'post-traumatic epilepsy' many years down the line. While there is no evidence yet as to the impact of TBI-induced epilepsy from the wars in Afghanistan and Iraq, this bill will ensure that we are prepared for that possibility,"
http://braininjury.blogs.com/braininjury/brain_injury_rehabilitation/index.html
The Murray-Craig bill authorizes $6 million annually for the Epilepsy Centers of Excellence to support clinical, research and education efforts surrounding the incidence of epilepsy among current and future veterans with head and brain injuries.
According to Senator Craig, "Experts have indicated that half of all Vietnam veterans who suffered penetrating brain injuries suffer from what is known as 'post-traumatic epilepsy' many years down the line. While there is no evidence yet as to the impact of TBI-induced epilepsy from the wars in Afghanistan and Iraq, this bill will ensure that we are prepared for that possibility,"
http://braininjury.blogs.com/braininjury/brain_injury_rehabilitation/index.html
Brain Blood Flow Gives Clues to Treating Depression
August 7, 2007
RESTON, Va.—The usefulness of established molecular imaging/nuclear medicine approaches in identifying the “hows” and “whys” of brain dysfunction and its potential in providing immediately useful information in treating depression are emphasized in a study in the August Journal of Nuclear Medicine.
“Individuals in a depressed emotional state have impaired cerebral (brain) blood flow,” explained Omer Bonne, head of inpatient psychiatry and associate professor in the Department of Psychiatry at Hadassah-Hebrew University Medical Center in Jerusalem, Israel. “Clinical improvement in depression is accompanied by diverse changes in cerebral blood flow, according to whether patients are treated with medication or electroconvulsive treatment,” he noted. “We found that antidepressant medicines normalized decreased brain blood flow usually seen in patients with depression, while electroconvulsive treatment was associated with additional decreases in blood flow,” he reported. “Currently, clinical psychiatry is based almost solely on subjective observer-based judgment. Our findings suggest that objective imaging evaluations could support subjective clinical decisions,” he said.
Using SPECT (single photon emission computed tomography)—a molecular imaging/nuclear medicine procedure in which injected radiotracers are utilized to produce three-dimensional, computer-reconstructed images that reveal information about both structure and function—investigators confirmed already published findings that cerebral blood flow in depressed patients is lower than in healthy control subjects, especially in frontal, limbic and subcortical brain regions. “We wanted to see whether improvement in clinical depression is accompanied by changes—increases—in cerebral blood flow,” he said. “We found that cerebral blood flow increased only in patients whose depression improved. In contrast, cerebral blood flow remained unchanged in patients whose depressed condition persisted,” detailed Bonne.
Depression is a serious and debilitating—yet treatable—disease that affects every aspect of a person’s health. Estimates indicate that 19 million Americans are affected by depression each year, along with their family members, friends and co-workers. Depression may be related to a chemical imbalance in the brain that makes it hard for the cells to communicate with one another. A variety of antidepressant medications and psychotherapies are used to treat depression. Sometimes electroconvulsive therapy—applying an electric current briefly to produce a seizure—is useful, especially for those whose depression is severe or life threatening or for whom repeated treatment trials with antidepressant drugs failed.
“Interestingly, patients’ response to two different classes of antidepressant medicines that target different neurotransmitters is associated with a similar improvement in cerebral blood flow,” he noted. “However, cerebral blood flow continued to deteriorate in patients who responded to electroconvulsive therapy,” added Bonne, who helped implement functional brain imaging research in psychiatry at Hadassah. Israeli researchers studied 33 depressed patients and 25 healthy control subjects with SPECT and the radiotracer 99mTc-HMPAO.
“Our findings may aid in elucidating the mechanism of depression and its treatment,” said Bonne. “There may be more than one mechanism responsible for the development of depression and for mediating response to its treatment,” he added. Additional research could examine whether it’s possible to use functional imaging techniques to determine which patients would benefit from drug treatment and which would respond better to electroconvulsive therapy, explained Bonne. Future research should also examine the differences in brain blood flow in patients at later time points, he said.
“99mTc-HMPAO SPECT Study of Cerebral Perfusion After Treatment With Medication and Electroconvulsive Therapy in Major Depression” appears in the August issue of the Journal of Nuclear Medicine, which is published by SNM, the world’s largest molecular imaging and nuclear medicine society. Co-authors include Yoav Kohn and Bernard Lerer, Department of Psychiatry, and Nanette Freedman, Hava Lester, Yodphat Krausz and Roland Chisin, Department of Medical Biophysics and Nuclear Medicine, at Hadassah-Hebrew University Medical Center in Jerusalem, Israel.
Media representatives: To obtain a copy of this article, please contact Maryann Verrillo by phone at (703) 652-6773 or send an e-mail to mverrillo@snm.org. Current and past issues of the Journal of Nuclear Medicine can be found online at http://jnm.snmjournals.org. Print copies can be obtained by contacting the SNM Service Center, 1850 Samuel Morse Drive, Reston, VA 20190-5316; phone (800) 513-6853; e-mail servicecenter@snm.org; fax (703) 708-9015. A subscription to the journal is an SNM member benefit.
http://interactive.snm.org/index.cfm?PageID=6645
RESTON, Va.—The usefulness of established molecular imaging/nuclear medicine approaches in identifying the “hows” and “whys” of brain dysfunction and its potential in providing immediately useful information in treating depression are emphasized in a study in the August Journal of Nuclear Medicine.
“Individuals in a depressed emotional state have impaired cerebral (brain) blood flow,” explained Omer Bonne, head of inpatient psychiatry and associate professor in the Department of Psychiatry at Hadassah-Hebrew University Medical Center in Jerusalem, Israel. “Clinical improvement in depression is accompanied by diverse changes in cerebral blood flow, according to whether patients are treated with medication or electroconvulsive treatment,” he noted. “We found that antidepressant medicines normalized decreased brain blood flow usually seen in patients with depression, while electroconvulsive treatment was associated with additional decreases in blood flow,” he reported. “Currently, clinical psychiatry is based almost solely on subjective observer-based judgment. Our findings suggest that objective imaging evaluations could support subjective clinical decisions,” he said.
Using SPECT (single photon emission computed tomography)—a molecular imaging/nuclear medicine procedure in which injected radiotracers are utilized to produce three-dimensional, computer-reconstructed images that reveal information about both structure and function—investigators confirmed already published findings that cerebral blood flow in depressed patients is lower than in healthy control subjects, especially in frontal, limbic and subcortical brain regions. “We wanted to see whether improvement in clinical depression is accompanied by changes—increases—in cerebral blood flow,” he said. “We found that cerebral blood flow increased only in patients whose depression improved. In contrast, cerebral blood flow remained unchanged in patients whose depressed condition persisted,” detailed Bonne.
Depression is a serious and debilitating—yet treatable—disease that affects every aspect of a person’s health. Estimates indicate that 19 million Americans are affected by depression each year, along with their family members, friends and co-workers. Depression may be related to a chemical imbalance in the brain that makes it hard for the cells to communicate with one another. A variety of antidepressant medications and psychotherapies are used to treat depression. Sometimes electroconvulsive therapy—applying an electric current briefly to produce a seizure—is useful, especially for those whose depression is severe or life threatening or for whom repeated treatment trials with antidepressant drugs failed.
“Interestingly, patients’ response to two different classes of antidepressant medicines that target different neurotransmitters is associated with a similar improvement in cerebral blood flow,” he noted. “However, cerebral blood flow continued to deteriorate in patients who responded to electroconvulsive therapy,” added Bonne, who helped implement functional brain imaging research in psychiatry at Hadassah. Israeli researchers studied 33 depressed patients and 25 healthy control subjects with SPECT and the radiotracer 99mTc-HMPAO.
“Our findings may aid in elucidating the mechanism of depression and its treatment,” said Bonne. “There may be more than one mechanism responsible for the development of depression and for mediating response to its treatment,” he added. Additional research could examine whether it’s possible to use functional imaging techniques to determine which patients would benefit from drug treatment and which would respond better to electroconvulsive therapy, explained Bonne. Future research should also examine the differences in brain blood flow in patients at later time points, he said.
“99mTc-HMPAO SPECT Study of Cerebral Perfusion After Treatment With Medication and Electroconvulsive Therapy in Major Depression” appears in the August issue of the Journal of Nuclear Medicine, which is published by SNM, the world’s largest molecular imaging and nuclear medicine society. Co-authors include Yoav Kohn and Bernard Lerer, Department of Psychiatry, and Nanette Freedman, Hava Lester, Yodphat Krausz and Roland Chisin, Department of Medical Biophysics and Nuclear Medicine, at Hadassah-Hebrew University Medical Center in Jerusalem, Israel.
Media representatives: To obtain a copy of this article, please contact Maryann Verrillo by phone at (703) 652-6773 or send an e-mail to mverrillo@snm.org. Current and past issues of the Journal of Nuclear Medicine can be found online at http://jnm.snmjournals.org. Print copies can be obtained by contacting the SNM Service Center, 1850 Samuel Morse Drive, Reston, VA 20190-5316; phone (800) 513-6853; e-mail servicecenter@snm.org; fax (703) 708-9015. A subscription to the journal is an SNM member benefit.
http://interactive.snm.org/index.cfm?PageID=6645
Brain Blood Flow Gives Clues to Treating Depression
August 11, 2007
A brief note on SPECT imaging for assessing depression from Israel: Keeping up with brain science.
This interesting press release from the Society of Nuclear Medicine makes it clear that the naysayers who don't get the significance of SPECT imaging in everyday psych practice need to rethink their tunneling position. We can see types of depression if we look. Here is a brief review:
The usefulness of established molecular imaging/nuclear medicine approaches in identifying the "hows" and €"whys" of brain dysfunction and its potential in providing immediately useful information in treating depression are emphasized in a study in the August Journal of Nuclear Medicine.
"€œIndividuals in a depressed emotional state have impaired cerebral (brain) blood flow," explained Omer Bonne, head of inpatient psychiatry and associate professor in the Department of Psychiatry at Hadassah-Hebrew University Medical Center in Jerusalem, Israel.
"Currently, clinical psychiatry is based almost solely on subjective observer-based judgment. Our findings suggest that objective imaging evaluations could support subjective clinical decisions."€ he said.
Sounds like what we have been saying, what Amen has been saying, for many years. Doesn't mean we have to run out and scan everybody, just that others do see the validity of the evidence.
The link above is only the press release, but links to the article are available there [above].
A brief note on SPECT imaging for assessing depression from Israel: Keeping up with brain science.
This interesting press release from the Society of Nuclear Medicine makes it clear that the naysayers who don't get the significance of SPECT imaging in everyday psych practice need to rethink their tunneling position. We can see types of depression if we look. Here is a brief review:
The usefulness of established molecular imaging/nuclear medicine approaches in identifying the "hows" and €"whys" of brain dysfunction and its potential in providing immediately useful information in treating depression are emphasized in a study in the August Journal of Nuclear Medicine.
"€œIndividuals in a depressed emotional state have impaired cerebral (brain) blood flow," explained Omer Bonne, head of inpatient psychiatry and associate professor in the Department of Psychiatry at Hadassah-Hebrew University Medical Center in Jerusalem, Israel.
"Currently, clinical psychiatry is based almost solely on subjective observer-based judgment. Our findings suggest that objective imaging evaluations could support subjective clinical decisions."€ he said.
Sounds like what we have been saying, what Amen has been saying, for many years. Doesn't mean we have to run out and scan everybody, just that others do see the validity of the evidence.
The link above is only the press release, but links to the article are available there [above].
http://www.corepsychblog.com/spectpet/index.html
Thursday, August 9, 2007
Abused No More

You may have thought you knocked me down and took me away,You controlled my body but not my mind With this mind I reclaim the power to unleash all the dirty deedsyou did to me Your dirty deeds are now sent free,The power you thought you had stolen from me was only hiding deep within So now it's my time for me to fly and make you squirm with mygoodbye to all the fears you unleashed on me so the world cansee the real me The power you gave me I thought was to hide in shame but now Icontrol the game, my pieces you can't remove for now I reclaimthe game you stole from meA kid filled world I never knew so take a seat and watch me playfor you thought you crushed me low so you could controlNow I'm standing crushing each fear you handed me, one by onethey come crashing down and when they fall I really seeyou made me fear it wasn't really meSo much shocking news I can really be meYour game is old and now I can see it wasn't me who had the fearyou hid behind the fear you used on meWords you knew I needed to hear those you manipulated to form yourgame are now being redefinedThe fog is lifted and now I see you robbed me of one promise onlya child can know, it's called innocenceMy eyes are set on a higher goal for revenge would be to easy,my revenge is therapy so I can reclaim the things you tookfrom me and when I'm done a box you will recieve filled withall your dirty deeds, for one day they will have no affect on me.
Kathy Austin
Welcome to the Baby Brain Map, a ZERO TO THREE Web exclusive
This website gives an understanding of how valueable our very young brains are and how damage can mis shape our brain.
To get started, select an age range from the pull-down menu and click on it. Depending on the age range, different hotspots on the brain will appear. Click on a hotspot to reveal questions to find out how a baby's brain develops during this period of brain growth. You'll also learn what you can do to enrich a very young child's development.
http://www.zerotothree.org/site/PageServer?pagename=ter_util_babybrainflash
It Shouldn’t Hurt To Be A Kid!
Yet, children continue to be hurt every
day. For these children there is no hope
unless each one of us realizes that our
most important duty is the protection,
welfare and growth of our children.
Child abuse can leave a scar that is carried
throughout life. In fact, statistics show
that the abused child all too often grows
up to be an abuser. We know that
breaking the cycle of abuse will not only
protect our children, but will reduce crime
now and in the future. Studies suggest
that 85 percent of convicted felons were
abused as children.
Without individual and community concern
and involvement, there are really three
“victims” of child abuse: the child, the
abuser, and the community. However,
each of us may make a valuable contribution
to the protection of children and the
prevention of abuse. Our concern and
involvement are critical — it may save a
life.
http://ci.santa-rosa.ca.us/images/Child%20Abuse.pdf
day. For these children there is no hope
unless each one of us realizes that our
most important duty is the protection,
welfare and growth of our children.
Child abuse can leave a scar that is carried
throughout life. In fact, statistics show
that the abused child all too often grows
up to be an abuser. We know that
breaking the cycle of abuse will not only
protect our children, but will reduce crime
now and in the future. Studies suggest
that 85 percent of convicted felons were
abused as children.
Without individual and community concern
and involvement, there are really three
“victims” of child abuse: the child, the
abuser, and the community. However,
each of us may make a valuable contribution
to the protection of children and the
prevention of abuse. Our concern and
involvement are critical — it may save a
life.
http://ci.santa-rosa.ca.us/images/Child%20Abuse.pdf
Instead of No what can we replace it with and not influence fear or control
These verbal social guidelines are influential, strong and effective. They have the ability to teach children without using power or control over them.
Principle 2: Respectful Information
Commands like the word "no" are harsh and build resistance in children. It is easier for children to hear how to do something correctly rather than to hear what they are doing wrong. More often than not, when given respectful information, children comply with social guidelines rather than resist them. Our language helps to mold a child's thoughts. "No" is a negative word and implies wrongdoing. It is also used to deny, refuse, or disagree. "No" is not meant to be flexible or compromising. You may have heard a popular saying, "What part of 'no' don't you understand?" This kind of language molds controlling and negative thoughts, which can be damaging to children. Every time you want to say no to a child, ask yourself what is not okay about the behavior
http://fatherhood.about.com/od/effectivediscipline/a/nonotforkids_2.htm?terms=child+abuse+power+point+presentation
Principle 2: Respectful Information
Commands like the word "no" are harsh and build resistance in children. It is easier for children to hear how to do something correctly rather than to hear what they are doing wrong. More often than not, when given respectful information, children comply with social guidelines rather than resist them. Our language helps to mold a child's thoughts. "No" is a negative word and implies wrongdoing. It is also used to deny, refuse, or disagree. "No" is not meant to be flexible or compromising. You may have heard a popular saying, "What part of 'no' don't you understand?" This kind of language molds controlling and negative thoughts, which can be damaging to children. Every time you want to say no to a child, ask yourself what is not okay about the behavior
http://fatherhood.about.com/od/effectivediscipline/a/nonotforkids_2.htm?terms=child+abuse+power+point+presentation
Wednesday, August 8, 2007
''The brains of adult survivors are fragmented and resemble a hard drive on a computer that has crashed.''
How child abuse and neglect damage the brain
Until recently, mental health clinicians could only speculate on the ways that abuse and neglect damage a child's developing brain. But a series of ground-breaking studies in neuroscience conducted over the last decade are allowing researchers to pinpoint the actual changes in children's brains caused by traumatic experience.
http://www.snapnetwork.org/psych_effects/how_abuse_andneglect.htm
Until recently, mental health clinicians could only speculate on the ways that abuse and neglect damage a child's developing brain. But a series of ground-breaking studies in neuroscience conducted over the last decade are allowing researchers to pinpoint the actual changes in children's brains caused by traumatic experience.
http://www.snapnetwork.org/psych_effects/how_abuse_andneglect.htm
Mindfulness
This brief introduction orients you to what is contained in the remaining sections of this page.
First, a message to those who will begin reading and find themselves thinking, "I can't see myself doing mindfulness meditation practices, so I might as well stop reading now and not bother coming back to this later":
Simply reading this page (whether or not you try meditating) will introduce you to new, and potentially very transformative and healing, ways of thinking about and experiencing your own mental and emotional processes. Just learning these concepts and points of view has proved extremely helpful to many people, including those with histories of significant child abuse. I can't guarantee that will happen for you, but I would like to encourage you to take the time, at some point, to find out for yourself.
http://www.jimhopper.com/mindfulness/#whatis
First, a message to those who will begin reading and find themselves thinking, "I can't see myself doing mindfulness meditation practices, so I might as well stop reading now and not bother coming back to this later":
Simply reading this page (whether or not you try meditating) will introduce you to new, and potentially very transformative and healing, ways of thinking about and experiencing your own mental and emotional processes. Just learning these concepts and points of view has proved extremely helpful to many people, including those with histories of significant child abuse. I can't guarantee that will happen for you, but I would like to encourage you to take the time, at some point, to find out for yourself.
http://www.jimhopper.com/mindfulness/#whatis
Addicted to Dopamine check it out !!!!!!!!!
Enjoyment triggers areas in your brain known as 'pleasure centres'. They release 'feel-good' chemicals, in particular dopamine
http://www.sciencemuseum.org.uk/exhibitions/brain/123.asp
http://www.sciencemuseum.org.uk/exhibitions/brain/123.asp
ReThink
The American Academy of Pediatrics recommends using what it calls the RETHINK method to bring your feelings under control. RETHINK stands for:
•R ecognize your feelings.
•E mpathize with your child.
•T hink of the situation differently. (Try using humor.)
•H ear what your child is saying.
•I ntegrate your love with your angry thoughts.
•N otice your body's reactions to feeling anger and to calming down.
•K eep your attention on the present problem.
A 1999 study at Colorado State University found that parents who participated in a six-week workshop based on this method became more effective at managing their anger.
http://www.ahealthyme.com/topic/verbalabuse
•R ecognize your feelings.
•E mpathize with your child.
•T hink of the situation differently. (Try using humor.)
•H ear what your child is saying.
•I ntegrate your love with your angry thoughts.
•N otice your body's reactions to feeling anger and to calming down.
•K eep your attention on the present problem.
A 1999 study at Colorado State University found that parents who participated in a six-week workshop based on this method became more effective at managing their anger.
http://www.ahealthyme.com/topic/verbalabuse
Remember
DISCIPLINE helps a child learn a lesson that will carry over and positively affect future behavior. ABUSE affects the future in a negative way, leading to anger, hatred and more deviant behavior.
DISCIPLINE enhances the child's sense of self worth, helping the child learn self-control and thus becoming comfortable within the family and in society. ABUSE robs the child of self worth and causes him/her to feel outcast and resentful.
DISCIPLINE is not shame or guilt. ABUSE is shame or guilt which satisfies the needs of the parents at the moment and destroys the self image of the child in a hostile manner.
DISCIPLINE is taught by example. But so is abuse!
Adapted from Child Discipline: Guidelines for Parents by Gary May.
http://www.nationalcac.org/families/for_workers/abuse_indicators.html
DISCIPLINE enhances the child's sense of self worth, helping the child learn self-control and thus becoming comfortable within the family and in society. ABUSE robs the child of self worth and causes him/her to feel outcast and resentful.
DISCIPLINE is not shame or guilt. ABUSE is shame or guilt which satisfies the needs of the parents at the moment and destroys the self image of the child in a hostile manner.
DISCIPLINE is taught by example. But so is abuse!
Adapted from Child Discipline: Guidelines for Parents by Gary May.
http://www.nationalcac.org/families/for_workers/abuse_indicators.html
How much does it cost a society to look away from the suffering of it's children?
Costs to SocietyIn a 1992, a state-level analysis of the costs associated with child maltreatment and its consequences was undertaken in Michigan. "These costs were then compared to the costs of providing child maltreatment prevention services to all first time parents. The costs of child abuse were estimated at 823 million dollars annually. These costs include those associated with low birthweight babies, infant mortality, special education, protective service, foster care, juvenile and adult criminality, and psychological services. The costs of prevention programming were estimated to be 43 million dollars annually. This yields a 19 to 1 cost advantage to prevention."
http://www.findcounseling.com/journal/child-abuse/abuse-neglect.html
http://www.findcounseling.com/journal/child-abuse/abuse-neglect.html
"A woman living her life in fear and abuse, can't raise a future generation that has Love, Understanding, Education, and Respect. STOP THE VIOLENCE.
Post traumatic stress disorder (PTSD) is used to describe the normal reactions of any person who has experienced an "abnormal," or extremely stressful, event. War veterans, survivors of natural disasters such as earthquakes, sexual abuse or rape survivors, and survivors of domestic violence all commonly experience PTSD.
Because of the on-going, predictable, and extremely stressful nature of a violent or abusive environment, just getting out of the abusive relationship does not end the emotional turmoil you feel. PTSD is a very common aftereffect for women and children who live or have lived in abusive relationships. The symptoms of PTSD can continue for more than a month or even last for years, and can begin from any time from immediately after to years after the traumatic event(s).
WomensCrisisline.org
http://womenscrisisline.org/ptsd.htm
Because of the on-going, predictable, and extremely stressful nature of a violent or abusive environment, just getting out of the abusive relationship does not end the emotional turmoil you feel. PTSD is a very common aftereffect for women and children who live or have lived in abusive relationships. The symptoms of PTSD can continue for more than a month or even last for years, and can begin from any time from immediately after to years after the traumatic event(s).
WomensCrisisline.org
http://womenscrisisline.org/ptsd.htm
"A woman living her life in fear and abuse, can't raise a future generation that has Love, Understanding, Education, and Respect. STOP THE VIOLENC
Post traumatic stress disorder (PTSD) is used to describe the normal reactions of any person who has experienced an "abnormal," or extremely stressful, event. War veterans, survivors of natural disasters such as earthquakes, sexual abuse or rape survivors, and survivors of domestic violence all commonly experience PTSD.
Because of the on-going, predictable, and extremely stressful nature of a violent or abusive environment, just getting out of the abusive relationship does not end the emotional turmoil you feel. PTSD is a very common aftereffect for women and children who live or have lived in abusive relationships. The symptoms of PTSD can continue for more than a month or even last for years, and can begin from any time from immediately after to years after the traumatic event(s).
WomensCrisisline.org
http://womenscrisisline.org/ptsd.htm
Because of the on-going, predictable, and extremely stressful nature of a violent or abusive environment, just getting out of the abusive relationship does not end the emotional turmoil you feel. PTSD is a very common aftereffect for women and children who live or have lived in abusive relationships. The symptoms of PTSD can continue for more than a month or even last for years, and can begin from any time from immediately after to years after the traumatic event(s).
WomensCrisisline.org
http://womenscrisisline.org/ptsd.htm
Q. What Are the Major Types of Child Abuse and Neglect?
From NCCANCH
A. Within the minimum standards set by CAPTA, each State is responsible for providing its own definitions of child abuse and neglect. Most States recognize four major types of maltreatment: neglect, physical abuse, sexual abuse, and emotional abuse. Although any of the forms of child maltreatment may be found separately, they often occur in combination.
The examples provided below are for general informational purposes only. Not all States' definitions will include all of the examples listed below, and individual States' definitions may cover additional situations not mentioned here.
Neglect is failure to provide for a child's basic needs. Neglect may be:
Physical (e.g., failure to provide necessary food or shelter, or lack of appropriate supervision)
Medical (e.g., failure to provide necessary medical or mental health treatment)
Educational (e.g., failure to educate a child or attend to special education needs)
Emotional (e.g., inattention to a child's emotional needs, failure to provide psychological care, or permitting the child to use alcohol or other drugs)
These situations do not always mean a child is neglected.
Sometimes cultural values, the standards of care in the community, and poverty may be contributing factors, indicating the family is in need of information or assistance. When a family fails to use information and resources, and the child's health or safety is at risk, then child welfare intervention may be required.
Physical Abuse is physical injury (ranging from minor bruises to severe fractures or death) as a result of punching, beating, kicking, biting, shaking, throwing, stabbing, choking, hitting (with a hand, stick, strap, or other object), burning, or otherwise harming a child. Such injury is considered abuse regardless of whether the caretaker intended to hurt the child.
Sexual Abuse includes activities by a parent or caretaker such as fondling a child's genitals, penetration, incest, rape, sodomy, indecent exposure, and exploitation through prostitution or the production of pornographic materials.
Emotional Abuse is a pattern of behavior that impairs a child's emotional development or sense of self-worth. This may include constant criticism, threats, or rejection, as well as withholding love, support, or guidance. Emotional abuse is often difficult to prove and, therefore, CPS may not be able to intervene without evidence of harm to the child. Emotional abuse is almost always present when other forms are identified.
http://parentingteens.about.com/cs/childabuse/f/childabuse2.htm
A. Within the minimum standards set by CAPTA, each State is responsible for providing its own definitions of child abuse and neglect. Most States recognize four major types of maltreatment: neglect, physical abuse, sexual abuse, and emotional abuse. Although any of the forms of child maltreatment may be found separately, they often occur in combination.
The examples provided below are for general informational purposes only. Not all States' definitions will include all of the examples listed below, and individual States' definitions may cover additional situations not mentioned here.
Neglect is failure to provide for a child's basic needs. Neglect may be:
Physical (e.g., failure to provide necessary food or shelter, or lack of appropriate supervision)
Medical (e.g., failure to provide necessary medical or mental health treatment)
Educational (e.g., failure to educate a child or attend to special education needs)
Emotional (e.g., inattention to a child's emotional needs, failure to provide psychological care, or permitting the child to use alcohol or other drugs)
These situations do not always mean a child is neglected.
Sometimes cultural values, the standards of care in the community, and poverty may be contributing factors, indicating the family is in need of information or assistance. When a family fails to use information and resources, and the child's health or safety is at risk, then child welfare intervention may be required.
Physical Abuse is physical injury (ranging from minor bruises to severe fractures or death) as a result of punching, beating, kicking, biting, shaking, throwing, stabbing, choking, hitting (with a hand, stick, strap, or other object), burning, or otherwise harming a child. Such injury is considered abuse regardless of whether the caretaker intended to hurt the child.
Sexual Abuse includes activities by a parent or caretaker such as fondling a child's genitals, penetration, incest, rape, sodomy, indecent exposure, and exploitation through prostitution or the production of pornographic materials.
Emotional Abuse is a pattern of behavior that impairs a child's emotional development or sense of self-worth. This may include constant criticism, threats, or rejection, as well as withholding love, support, or guidance. Emotional abuse is often difficult to prove and, therefore, CPS may not be able to intervene without evidence of harm to the child. Emotional abuse is almost always present when other forms are identified.
http://parentingteens.about.com/cs/childabuse/f/childabuse2.htm
Tuesday, August 7, 2007
The Neurocritic
Deconstructing the most sensationalistic recent findings in Human Brain Imaging, Cognitive Neuroscience, and Psychopharmacology
http://neurocritic.blogspot.com/2006/06/are-you-conscious-of-your-precuneus.html
http://neurocritic.blogspot.com/2006/06/are-you-conscious-of-your-precuneus.html
Monday, August 6, 2007
The Soul in the Brain
The Cerebral Basis of Language, Art, and Belief
DescriptionIn this provocative study, Michael R. Trimble, M.D., tackles the interrelationship between brain function, language, art—especially music and poetry—and religion. By examining the breakdown of language in several neuropsychiatric disorders, neuroscientists have identified brain circuits that are involved with metaphor, poetry, music, and religious experiences. Drawing on this body of evidence, Trimble argues that religious experiences and beliefs are explicable biologically and relate to brain function, especially of the nondominant hemisphere. Inspired by the writings and reflections of his patients—many of whom have epilepsy, psychosis, or affective disorders—Trimble asks how the human species, so enamored of its own logic and critical facilities, has held from the dawn of civilization strong religious beliefs and a reverence for the arts. He explores topics such as the phenomena of hypergraphia and hyper-religiosity, how religious experiences and poetic expression are neurologically linked with our capacity to respond to music, and how neuropsychiatric disorders influence behaviors related to artistic expression and religiosity by disturbing brain function. With the sensitivity of a dedicated doctor and the curiosity of an accomplished scholar, Trimble offers an insightful analysis of how the study of people with paradigmatical neuropsychiatric conditions can be the cornerstone to unraveling some of the mysteries of the cerebral representations of our highest cultural experiences.
http://www.press.jhu.edu/books/title_pages/3293.html
DescriptionIn this provocative study, Michael R. Trimble, M.D., tackles the interrelationship between brain function, language, art—especially music and poetry—and religion. By examining the breakdown of language in several neuropsychiatric disorders, neuroscientists have identified brain circuits that are involved with metaphor, poetry, music, and religious experiences. Drawing on this body of evidence, Trimble argues that religious experiences and beliefs are explicable biologically and relate to brain function, especially of the nondominant hemisphere. Inspired by the writings and reflections of his patients—many of whom have epilepsy, psychosis, or affective disorders—Trimble asks how the human species, so enamored of its own logic and critical facilities, has held from the dawn of civilization strong religious beliefs and a reverence for the arts. He explores topics such as the phenomena of hypergraphia and hyper-religiosity, how religious experiences and poetic expression are neurologically linked with our capacity to respond to music, and how neuropsychiatric disorders influence behaviors related to artistic expression and religiosity by disturbing brain function. With the sensitivity of a dedicated doctor and the curiosity of an accomplished scholar, Trimble offers an insightful analysis of how the study of people with paradigmatical neuropsychiatric conditions can be the cornerstone to unraveling some of the mysteries of the cerebral representations of our highest cultural experiences.
http://www.press.jhu.edu/books/title_pages/3293.html
Friday, August 3, 2007
NANCY GRACE
NANCY GRACE, HOST: Tonight, breaking news out of Charleston, South Carolina, the suburbs. A 27-year-old mother of two taken from the local hospital dressed in hospital scrubs and handcuffed, escorted straight to jail. Why? Police say 1-year-old Triniti, 4-year-old Shawn died a painful death when left trapped in soaring temperatures in mom`s car. Accident? Hold on! After mom makes a solo run to Arby`s for her own dinner, police find the children in garbage bags dead under the kitchen sink. Hope you enjoyed that roast beef sandwich, Mom, because it`s jail food tonight!(BEGIN VIDEO CLIP)UNIDENTIFIED MALE: Shocking details in the case of two kids who died after sitting in a hot car while their mother worked just steps away. The dead bodies of 4-year-old Shawn and 1-year-old Triniti were washed and dressed before being wrapped in trash bags, according to arrest warrants. A pathologist believes the kids were probably dead from heat exposure before they were washed, dressed and thrown under the sink next to a bag of garbage.(END VIDEO CLIP)GRACE: And tonight, a high-profile editor of a major Oakland newspaper gunned down execution-style on a public street as he, like the rest of us, simply walked to work that morning. The newspaper superstar, 57-year-old Chauncey Bailey (ph), now believed by police to be the victim of a hired hitman. But why?(BEGIN VIDEO CLIP)UNIDENTIFIED FEMALE: Chauncey Bailey, a long-time journalist who was shot to death yesterday in the heart of downtown Oakland. Fifty-eight- year-old Bailey was walking to work yesterday morning on 14th and (INAUDIBLE) Streets when he was gunned down. He most recently served as editor of "The Oakland Post." SWAT teams made entry into that one business called Your Black Muslim Bakery. It`s on the 5800 block of San Pablo (ph) Avenue. They say this stems out of a year-long investigation, including murder and robbery, several violent crimes.UNIDENTIFIED MALE: The search warrant yielded several weapons and other evidence of value, including evidence linking the murder of Chauncey Bailey to members of the Your Black Muslim Bakery.(END VIDEO CLIP)GRACE: Good evening. I`m Nancy Grace. I want to thank you for being with us tonight.First to South Carolina -- her two children found dead under the kitchen sink, left alone in a stifling hot car while mom goes to work, the temperatures soaring there in Charleston, South Carolina. But that`s not the end of it. Her two children apparently dead, and she heads to dinner at Arby`s?(BEGIN VIDEO CLIP)UNIDENTIFIED MALE: Now, police sayUNIDENTIFIED MALE: We responded to a disturbance at the Villa (ph) Apartments on Reenout (ph) Road. Officers arrived on scene. They saw a female in a struggle with an unknown subject. That male directed the officers to check inside the cabinet, at which time the bodies of two small children were discovered.UNIDENTIFIED MALE: Early speculation is that, you know, she took the children with her to work, didn`t have any care for the children, and left them in the car. That`s one possible, you know, instance that we`re investigating.(END VIDEO CLIP)GRACE: OK, let me get this straight. After the two children, toddlers ages 1 and 4, are dead, apparently from heat exhaustion there in the car, heat stroke, she then bathed them, washed them and meticulously dressed them before putting them out with the garbage?Out to Marika Kelderman, reporter with WCSC-TV joining us from Charleston. Marika, explain. What`s the latest?MARIKA KELDERMAN, WCSC-TV: Well, the big news today, Nancy, was that two psychiatrists were actually with the children`s mother, Sametta Heyward, just hours ago. They were brought in by her defense attorney to start on a mental evaluation that he actually says could take several weeks to complete. They want to do a full history to find out what her mental status was.Now, this was going on at the exact same time that a visitation was being held for her two children, Shawn Campbell, Jr., and his sister, Triniti. Their funeral is going to be held tomorrow. And we`ve actually learned their mother has been barred from attending the funeral and a judge actually denied a special request to have a private visitation for her so that she could say good-bye to her children. That`s the latest.GRACE: Well, I think she had plenty of time to say good-bye while they were out in her car for about, let`s just say, eight hours in the stifling heat! Now -- now, hold on. Here we go. Second verse, same as the first. The defense is already bringing in psychiatrists to try and develop an insanity defense.Let me go straight to Bethany Marshall, psychotherapist and author. Bethany, give it to me straight. And remember, you haven`t been hired by the defense, all right? This is a mom that worked her shift normally at work, no indication of mental illness, leaves the kids locked in the car, when she couldn`t -- didn`t try, I don`t know, or couldn`t get -- a baby- sitter, then comes home, bathes them, clothes them, goes out to Arby`s, and according to this police investigation report, calls an ex and says, I killed my babies. Now, where`s the insanity?BETHANY MARSHALL, PSYCHOANALYST: OK. Well, the fact that she called the ex and said, I killed my babies, means that she does know right from wrong. Here`s what I would be evaluating for. You have to look at socio- economic status. She was probably terrified to not show up for work, afraid of losing her job...GRACE: Wait. Did you just you tell me insanity depends on your socio-economic status?MARSHALL: No. No, no, no. That`s not what I said. I said...GRACE: Because I would have been crazy working in law school working those three jobs.MARSHALL: Hey, no, what I said was the fact that she called her ex says that she does know right from wrong. She called her ex and said, I killed my babies. That`s not insanity. This is something a little different, fear of losing her job. I would wonder if you have an ultra- conforming personality, panic, low ego strength, and I would want to do some psych testing to see if she has problems in the frontal lobe because people...GRACE: Whoa, whoa, whoa, whoa, whoa!MARSHALL: What that means, this is the part of the brain that`s the center of higher reasoning. And people who have problems in that area, when they panic, they cannot engage in linear causal or cause-and-effect thinking. So such as, How am I going to feed my babies? What`s going to happen if they need to go to the bathroom, if they need food, that kind of stuff.
http://transcripts.cnn.com/TRANSCRIPTS/0708/03/ng.01.html
http://transcripts.cnn.com/TRANSCRIPTS/0708/03/ng.01.html
Wednesday, August 1, 2007
My life has changed today
Today my life was made richer, today my life changed forever, today I learned to let down the wall of imprisonment and let in some goodness. Abuse has made my life a cobweb of confusion I have the potiental to reach any corner of the world but my first years in this world I was robbed of that chance. Thanks to a wonderful person who has led the way to open my world and slowly help me climb out and reach out and take in wonderful things. I am like a young butterfly awaiting on wings only to discover we all come with wings now I am in training to understand how my wings work so follow me on my journey and see how far I can fly.
Subscribe to:
Comments (Atom)

http://www.windyweb.com/stop.htm














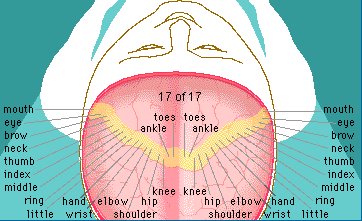
{kind=link}